Spinal pain in the lumbar region (lower back) and cervical region (neck) are highly prevalent and are often the causes for many lost work days. Lumbar muscle strains and sprains are the most common causes of low back pain. The thoracic spine can also be a site of spinal pain, but because it is much more rigid, the thoracic spinal area is much less frequently injured than the lumbar and cervical spine.
The lumbar and cervical spine are prone to strain because of its weight-bearing function and involvement in moving, twisting and bending. Lumbar muscle strain is caused when muscle fibers are abnormally stretched or torn. Lumbar sprain is caused when ligaments — the tough bands of tissue that hold bones together — are unusually stretched. Both of these can result from a sudden injury or from gradual overuse.
When the lumbar spine is strained or sprained, the soft tissues become inflamed. This inflammation causes pain and may cause muscle spasms. Even though lumbar strain or sprain can be very debilitating, neither usually requires neurosurgical attention.
Spinal pain can be caused by things more severe that might require surgical consideration. These usually involve spinal pain that radiates into arms, legs or around the rib cage from back toward the anterior chest.
Three types of muscles support the spine:
- Extensors (back muscles and gluteal muscles)
- Flexors (abdominal muscles and iliopsoas muscles)
- Oblique or rotators (side muscles)
SYMPTOMS + TYPES
Non-surgical low back, cervical and thoracic pain usually affects the central or para-spinal soft tissue without radiating into the arms, around the chest or down the legs. On the contrary, pain radiating from the spine into the extremities or chest wall implies structural pinching of the nerves in the spine that might require a surgical opinion if the situation fails to improve within days to weeks with non-surgical symptomatic treatment.
Other symptoms include:
- Stiffness in the low back area, restricting range of motion
- Inability to maintain normal posture due to stiffness and/or pain
- Muscle spasms either with activity or at rest
- Pain that persists for a maximum of 10-14 days
- Notable loss of motor function such as the ability to tiptoe or heel walk.
Herniated Disc Symptoms
Symptoms vary greatly depending on the position of the herniated disc and the size of the herniation. If the herniated disc is not pressing on a nerve, the patient might experience spinal pain (cervical, lumbar and/ or thoracic) or no pain at all. If there is pressure on a nerve, there can be pain, numbness or weakness in the area of the body to which the nerve travels. Typically, a herniated disc is preceded by an episode of spinal pain (cervical, lumbar and/or thoracic) or a long history of intermittent episodes of spinal pain.
Lumbar spine (lower back) — Sciatica frequently results from a herniated disc in the lower back. Pressure on one or several nerves that contribute to the sciatic nerve can cause pain, burning, tingling and numbness that radiates from the buttock into the leg and sometimes into the foot. Usually one side (left or right) is affected. This pain is often described as sharp and electric shock-like. It may be more severe with standing, walking or sitting. Along with leg pain, the patient may experience low back pain. Using the term radiculopathy may be more appropriate, rather than using the term sciatica, since all leg pain isn’t necessarily “sciatica.”
Cervical spine (neck) — Symptoms may include dull or sharp pain in the neck or between the shoulder blades that radiates down the arm to the hand or fingers, or numbness or tingling in the shoulder or arm. The pain may increase with certain positions or movements of the neck.
Thoracic spine — Symptoms of a thoracic disc herniation can be comprised of posterior chest pain radiating around one or both sides of the rib cage. Such pain is usually triggered by physical exertion and can even be caused by taking a deep breath. Bands of numbness around the chest wall can also be present. Herniated discs of the thoracic spine are relative rare compared to cervical and lumbar disc herniations.
TESTING + DIAGNOSIS
Diagnostic Testing
Diagnostic testing is usually necessary only when the pain has been present for more than two weeks and has not improved as expected. Likewise, if pain radiates into the extremities or around the chest well past the spinal epicenter of the pain focus, it is important to rule out underlying causes such as an undetected spinal disc injury. If symptoms are persistent, the following tests may be ordered by your doctor. It is important to note that regardless of diagnosis, an improving clinical picture supports continuing with nonsurgical modalities. If the improvement fails to reach a satisfactory stable point additional diagnostic efforts should be pursued. Likewise, if clinical symptoms deteriorate the diagnostic evaluation needs to be extended.
X-ray — Application of radiation to produce a film or picture of a part of the body can show the structure of the vertebrae and the outline of the joints. X-rays of the spine are obtained to search for other potential causes of pain; i.e. spinal malalignment, tumors, infections, fractures, etc.
Magnetic resonance imaging (MRI) — A diagnostic test that produces three-dimensional images of body structures using powerful magnets and computer technology. MRIs can show the spinal cord, nerve roots and surrounding areas, as well as enlargement, degeneration and tumors. Add contrast to the study and it can be made sensitive enough to detect inflammatory processes such as infections and new compression fractures without spinal malalignment.
CT scan with 3-D reconstruction —Shows boney detail better than any other imaging test and can still show soft tissue and nerves.
Electromyography or nerve conduction velocity testing — EMG/NCV neurophysiologic testing of nerves to help localize site of compression or other neural pathology.
TREATMENT + CARE
Non-surgical
Strains, sprains and even structural neural compression from disc herniations can be treated with diminished activity and even bed rest for a short period of time; usually from one to three days.
This should be as brief as possible, as prolonged bed rest can lead to a loss of muscle strength and may increase muscle stiffness, adding to pain and discomfort. Initial medical treatment is commonly comprised of nonsteroidal anti-inflammatory (NSAIDs) medication if the pain is mild to moderate. Muscle relaxants and narcotic medication can be added or substituted for cases of more severe pain symptoms.
The doctor may recommend physical therapy. The therapist will perform an in-depth evaluation, which combined with the doctor’s diagnosis, will dictate a treatment specifically designed for patients with spinal pain. Therapy may include pelvic traction, gentle massage, ice and heat therapy, ultrasound, electrical muscle stimulation and stretching exercises.
Prognosis
PREVENT + MANAGE
Prevention Tips
The following tips may be helpful in preventing low back pain associated with strain and sprain:
- Do crunches and other abdominal-muscle strengthening exercises to provide more spine stability. Swimming, stationary bicycling and brisk walking are good aerobic exercises that generally do not put extra stress on your back;
- Use correct lifting and moving techniques, such as squatting to lift a heavy object (don’t bend and lift). Get help if an object is too heavy or awkward;
- Maintain correct posture when you’re sitting and standing;
- Quit smoking. Smoking is a risk factor for atherosclerosis (hardening of the arteries), which can cause lower back pain and degenerative disc disorders;
- Avoid stressful situations if possible, as this can cause muscle tension;
- Maintain a healthy weight. Extra weight, especially around the midsection, can put strain on the lower back.
Surgical
Causes of surgically significant spine pain:
A single excessive strain or injury may cause a herniated disc. However, disc material degenerates naturally as people age, and the ligaments that hold it in place begin to weaken. As this degeneration progresses, a relatively minor strain or twisting movement can cause a disc to rupture.
Certain individuals may be more vulnerable to disc problems and, as a result, may suffer herniated discs in several places along the spine. Research has shown that a predisposition for herniated discs may exist in families, with several members affected. This does not necessarily mean that disc disease is a hereditary condition but it can run in families.
Post Surgery
The surgeon will give the patient specific instructions following surgery and usually will prescribe pain medication. Sometimes a spinal brace will be applied for weeks to months depending on the specific postsurgical needs. The surgeon will help determine when normal activities such as returning to work, driving and exercising may resume. Some patients may benefit from supervised rehabilitation or physical therapy after surgery. Such treatment will usually require a referral.
Discomfort is expected while the patient gradually return to normal activity, but pain is a warning signal that the patient might need to slow down. In general, continued gradual improvement is the expected trend over the first three or more months following surgery. The surgeon will provide prognostic information and give an idea of how to determine what adverse post-operative trends necessitates scheduling an unplanned re-evaluation. Such adverse trends would include fever, chills, wound drainage, new weakness, sensory or pain symptoms.
Finally, a patient needs to know beforehand that there usually are no absolutes regarding medical or surgical treatment of spinal conditions. Every patient is unique. It can be confusing which treatment or which elective operation is best in each situation. That is why patients have to rely on choosing a physician carefully. This applies to non-surgeons as well as surgeons. Pick a doctor that the patient feels comfortable with regardless of ultimate outcome. The best physicians are the ones that a patient can trust to tough it out with them when the treatment outcome fails to be ideal.
Resources
Surgical Terms
Artificial disc surgery (disc arthroplasty)
Surgical replacement of a diseased or herniated cervical or lumbar disc with an artificial disc designed to maintain spinal mobility. These usually consist of a plastic core between two metallic (usually titanium) plates that lock into the spine (see Figures 1, 2 and 3).
Lumbar disc arthroplasty
Figure 1: (Left side) — L5-S1 lumbar disc herniation; (Right side) — L5-S1 disc arthroplasty

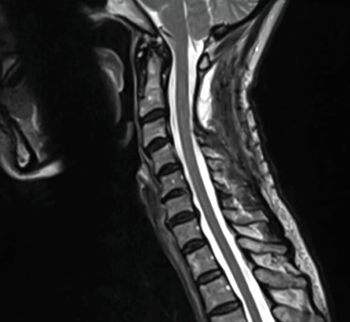
Cervical disc herniation and arthroplasty
Figure 2: (Left side) — C4-5-6-7 disc bulges most severe at transverse line (C5-6 level); (Right side) — arrow marks narrowing of the right nerve canal causing right arm pain due to C6 nerve root compression.
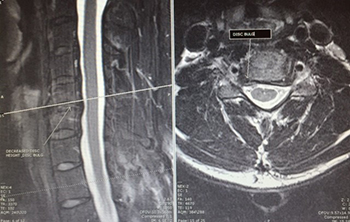
Figure 3: Post operative cervical disc replacement surgery showing motion preservation in neutral (left), flexion (middle) and extension (right) views on plain X-ray.

Discectomy
Surgical removal or partial removal of a herniated intervertebral disc.
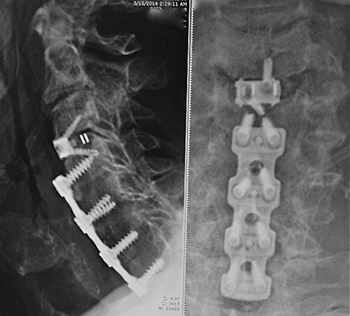
Figure 4: (Left side) = lateral and (Right side) = anterior-posterior. Plain X-rays showing long lower anterior cervical plate with more recent no profile intradiscal implant required for progression of disc disease above the prior fusion (“next segment disc disease”).
Cervical Discectomy
Patients with cervical disc herniation (as shown in Figure 2 above) that require surgery most often undergo anterior cervical discectomy with fusion (ACDF). This procedure requires the surgeon to operate through the front of the neck and can be performed using many types of implants including anterior titanium metallic plates and screws or intra-discal implants not requiring anterior plating (low or no profile implants). These implants are made of titanium, plastic or a combination (See Figure 4 on the left, of a case using a long anterior cervical titanium plate C4-5-6-7 in his first operation followed years later by a no profile implant at C3-4).
Other less commonly used procedures include anterior and posterior microdiscectomy usually without fusion. Some cases of extensive cervical stenosis require decompressive posterior laminectomy or laminoplasty augmented often by instrumented posterior cervical fusions (titanium rods, screws, plates). Alternatively, even these types of cases can be performed from the front of the neck and the surgery is called a corpectomy, with instrumented or metallic cage fusion.
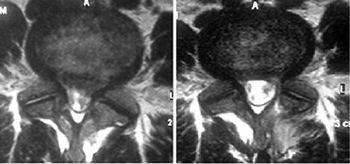
Figure 5: (Left side) Pre-op lumbar disc herniation; (Right side) Post-op lumbar microdiscectomy.
Lumbar Discectomy
Patients with lumbar disc herniation (as shown in Figure 1) that require surgery are most commonly treated with micro-discectomy or other minimally invasive techniques to simply remove the herniated disc without destabilizing the spine. The indications to perform this procedure or others can be confusing and requires clear communication between patient and surgeon.
Second opinions can be helpful but can also add to the confusion if first and second opinions conflict with each other. Figure 5 on the left shows axial views of before (left side) and after microdiscectomy (right side).
Another surgeon might have performed a total disc replacement which could have been as equally appropriate and effective.
Laminectomy
Surgical removal of most of the bony arch, or lamina of a vertebra for general decompression of neural elements with or without discectomy.
Laminotomy
An opening made in a lamina, to allow surgical access to relieve pressure on the neural elements such as nerve roots by removal of bone spurs and disc herniations as in Figure 5 above.
Spinal Fusion
Figure 6A (left): Spondylolysis with spondylolisthesis (spinal malalignment)
Often after decompression of the neural elements the spinal stability needs to be improved. This is particularly so in certain spinal diseases that imply spinal instability even before surgical treatment is provided; i.e., spondylolisthesis (see Figure 6A on the left). Stabilizing surgical procedures are commonly referred to as spinal fusion and can be performed in many ways.

Generally, bone is grafted onto or into the spine, creating a solid union between two or more vertebrae; and in which metallic (usually titanium) instrumentation such as plates, screws and rods may be used to provide additional spinal support. Such internal support can be thought of as an internal brace to support the spine while the natural fusion takes place and matures. The use of metal in the fusion is often referred to as an “instrumented fusion” (see Figure 6B).
In order to improve the probability of successful fusion, the surgeon might use bone harvested from the patient, allograft (processed cadaveric bone made safe for surgical use) and biochemical fusion enhancing substances (for example: demineralized bone matrix and human bone morphogenic protein or BMP). A successful fusion usually takes a minimum of three months and can take as long as a year or more to mature.
Figure 6B (left): Shows anterior — posterior view (left side) and lateral view (right side) of a case treated with PLIF — or Posterior Lumbar Interbody Fusion.

Spinal compression fracture
Figure 7: Showing lateral (left side) and anterior-posterior views (right side) of lumbar 5 compression fracture due to osteoporosis.
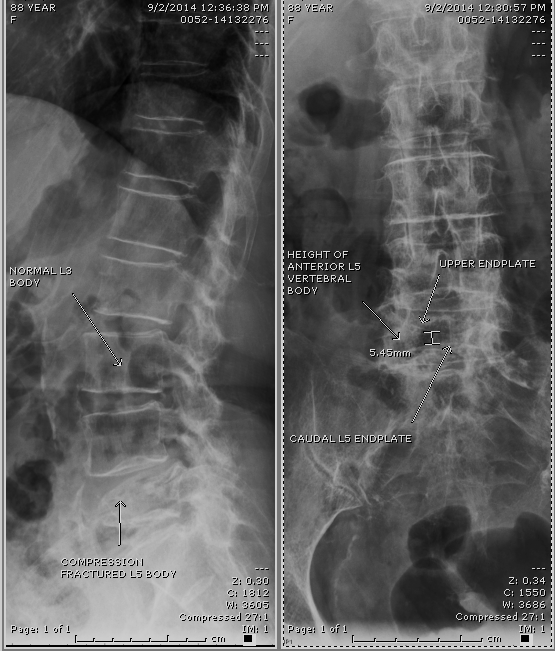
Patients with decreased calcium content can sustain vertebral body collapse with normal activities of daily living (see Figure 4). This usually causes the acute onset of moderate to severe spinal pain and can be treated with a back brace and pain medication, injection of the collapsed vertebrae with plastic (vertebroplasty and kyphoplasty) or open surgery, in selective cases (see Figure 7 on the left).
References
- Journal of Neurosurgery AAMarch 1990 / Vol. 72 / No. 3 / Pages 370-377: Posterolateral microdiscectomy for cervical monoradiculopathy caused by posterolateral soft cervical disc sequestration; Francois Aldrich, M.D., M.Med., F.C.S.– Division of Neurosurgery, The University of Texas Medical Branch, Galveston, Texas Address reprint requests to: Francois Aldrich, M.D., Division of Neurosurgery E-17, The University of Texas Medical Branch, Galveston, Texas 77550.
- Journal of Neurosurgery: Spine Aug 2012 / Vol. 17 / No. 2 / Pages 124; Unilateral surgical approach for lumbar disc herniation with contralateral symptoms Taşkan Akdeniz, M.D.1et.al. 1Department of Neurosurgery, Küçükyalı Delta Hospital; 2Department of Neurosurgery, Pendik State Hospital; 3Department of Neurosurgery, Fatih Sultan Mehmet Education and Training Hospital; and 4Department of Neurosurgery, American Hospital, Istanbul, Turkey
Note from AANS
The AANS does not endorse any treatments, procedures, products or physicians referenced in these patient fact sheets. This information is provided as an educational service and is not intended to serve as medical advice. Anyone seeking specific neurosurgical advice or assistance should consult his or her neurosurgeon, or locate one in your area through the AANS’ Find a Board-certified Neurosurgeon online tool.