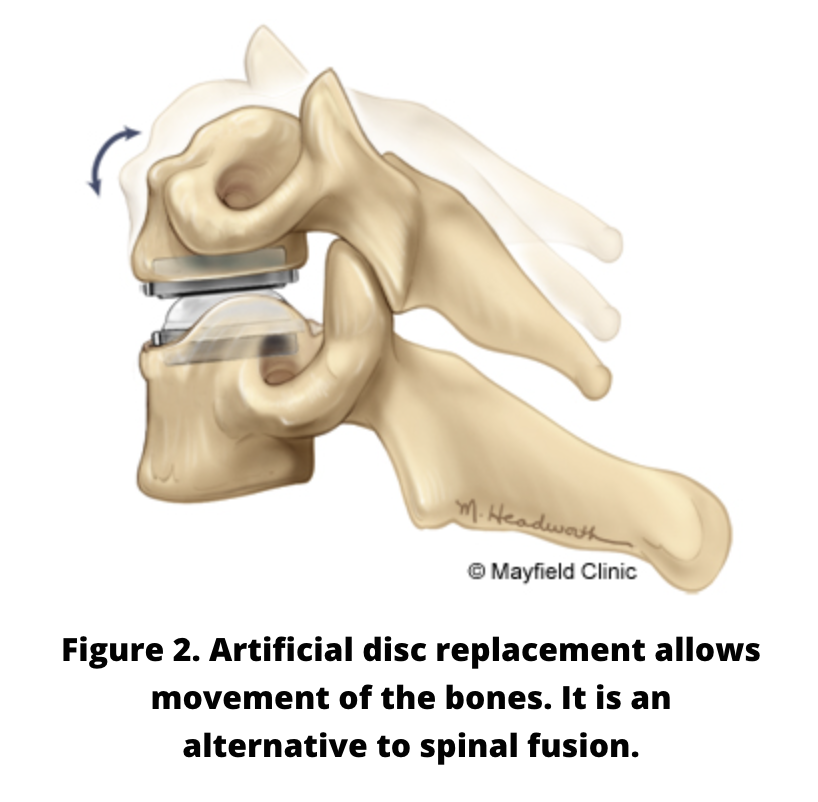
An artificial cervical disc seeks to replace the movement and cushioning function of damaged cervical disc.
Overview
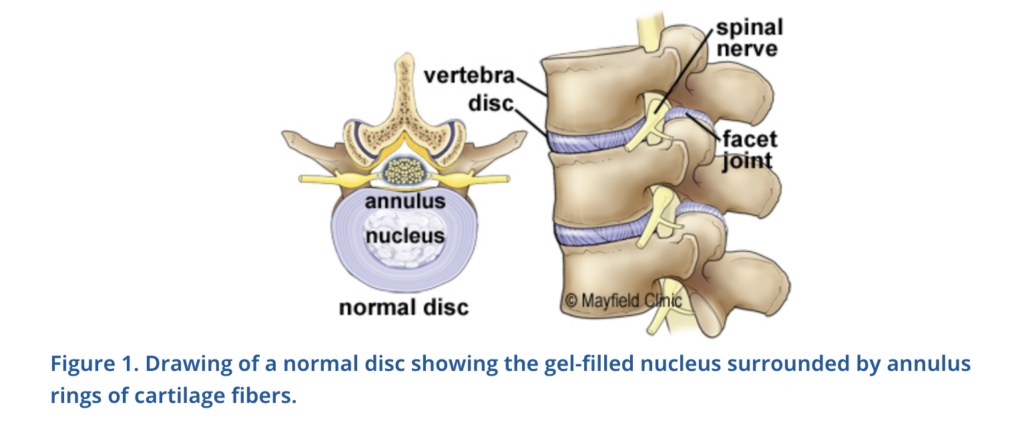
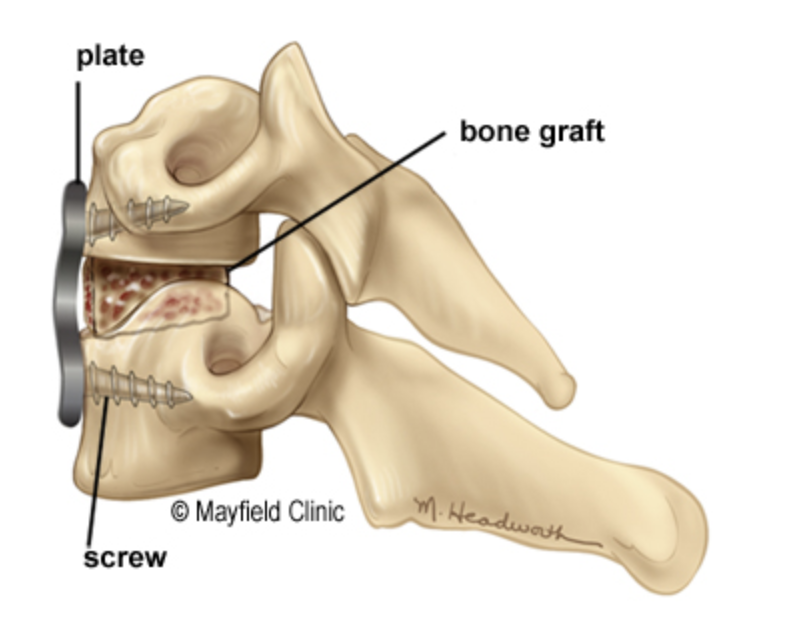
Cervical disc disease can cause neck pain or pain in the nerves of the arm and shoulder. The standard surgery seeks to replace the disc with any number of devices, the end goal being to fuse the upper and lower vertebral body. Theoretically, creating a solid piece of bone where two bones once moved independently accelerates degeneration of the discs above and below the fusion, also known as adjacent level disease. An artificial disc that seeks to mimic the properties of a healthy disc might alleviate these problems.
In comparison to spinal fusion surgery, potential benefits of artificial disc technology include more spine mobility after surgery and less stress on adjacent discs. While cervical artificial discs have been shown to preserve motion at the operated segment in most patients, their effectiveness in reducing the rate of symptomatic adjacent disc problems has not been established.
Symtoms + Types
Symptoms of cervical disc degeneration include neck pain and pain down one arm. If the patient has had a previous fusion, adjacent level disease would present with the new onset of similar symptoms.
WATCH CERVICAL RADICULOPATHY VIDEO
Treatment + Care
If neck pain accompanied by arm pain is present, consult with a spine surgeon. Often rest and therapy are prescribed to see if the symptoms can be alleviated without surgery.
To be considered a candidate for an artificial cervical disc, you must meet the following specific criteria:
- Disc degeneration in one or two cervical spine discs that are herniating and compressing nerve roots causing arm pain
- Failed conservative treatment, such as physical therapy, pain medication or neck bracing, without showing improvement
- Overall good health with no signs of infection, osteoporosis, arthritis or osteomalacia
- No known allergies to metals
If degeneration affects more than one disc, segmental instability or any type of metabolic or hereditary/acquired bone disease, the individual is not a candidate for this surgery. This surgery is not recommended in patients who have undergone prior spinal fusion/surgical procedures at the same or adjacent cervical levels.
During surgery, the patient is under general anesthesia and a small incision is made in the front of the neck. Through this opening, the affected disc is removed and replaced. The average postoperative hospital stay is one to two days. Although a similar artificial cervical disc has been used in Europe since 2004, there is little information available on the number of surgeries performed to date.
Potential Complications
- Need for additional surgery
- Allergic reaction to the implant materials
- Bleeding; may require a blood transfusion
- Blood vessel problems other than bleeding
- Death
- Development or progression of disease at other cervical levels
- Implants that bend, break, loosen or move
- Incision problems
- Infection
- Loss of motion at the treated cervical level
- Numbness or tingling in the extremities
- Pain or discomfort
- Paralysis
- Side effects from anesthesia
- Spinal cord or nerve damage
- Spinal fluid leakage
- Tears of the dura (a layer of tissue covering the spinal cord)
Prevent + Manage
It is routine to have immediate postoperative x-rays to confirm proper position of the device and alignment of the spine. Further imaging is often not needed without the appearance of new symptoms.
Resources
A 2016 meta-analysis of artificial cervical disc versus standard cervical fusion shows artificial disc patients with decreased evidence of adjacent level disease at four years of follow-up. The value of artificial disc surgery over standard fusion beyond that timeframe is uncertain and the subject of ongoing investigation.
Authors
Patient Pages are authored by neurosurgical professionals, with the goal of providing useful information to the public.
Neel T. Patel, MD, Neurosurgery Resident at the Penn State College of Medicine at the Milton S. Hershey Medical Center in Hershey, Penn.
Scott D. Simon, MD, FAANS, is an associate professor of neurosurgery at the Penn State College of Medicine at the Milton S. Hershey Medical Center in Hershey, Penn. He specializes in cerebrovascular and endovascular neurosurgery and his research interests include cerebrovascular device design and retro-viral delivered gene therapy for neural regeneration.
Note from AANS
The AANS does not endorse any treatments, procedures, products or physicians referenced in these patient fact sheets. This information is provided as an educational service and is not intended to serve as medical advice. Anyone seeking specific neurosurgical advice or assistance should consult his or her neurosurgeon, or locate one in your area through the AANS’ Find a Board-certified Neurosurgeon online tool.